Editor’s note: The findings and conclusions in this article are those of the author and do not necessarily represent the official position of the National Institute for Occupational Safety and Health or Centers for Disease Control and Prevention.
As you drive through the various suburbs in the U.S., an even more common sight than a white picket fence is a steep-slope roof. Depending where you are, the steepness can vary based on local climate or the year the house was constructed. Newer homes tend to have steeper roofs than their predecessors; this may be because of weather and/or for aesthetic purposes. Although the steeper-sloped roofs can add curb appeal, their construction can cause health and safety issues for those who install them.
Construction workers face many injury risks ranging from the traumatic (such as falling from heights or being struck by objects) to the repetitive or cumulative (such as musculoskeletal). Working on a residential (steep-slope) roof is no different but with the added element of a sloped working surface. Residential roofing workers have the second-highest incidence rate of not only injuries and fatalities but also work-related musculoskeletal disorders among all construction sectors based on data from the Bureau of Labor Statistics. Residential roofing workers can have prolonged exposures to awkward and static postures in which they crawl, squat, stoop and kneel.
In addition, these workers are required to perform manual material handling tasks such as carrying heavy materials and tools while on a sloped surface. Residential roofing workers also are exposed to repetitive motion, forceful exertion and impact vibration, for example, from nail gun operation.
Physical risks
Musculoskeletal injuries are a group of painful disorders that affect soft tissues (muscles, tendons and/or nerves) of the body. Although these ailments can affect any part of the body, for residential roofing workers the most common areas affected are their lower extremities (ankles, knees and hips) and/or their backs and spines. What makes musculoskeletal injuries such a problem is many people do not know they are at risk until they start to feel the effects of an injury. This happens because musculoskeletal injuries take time to develop and surface. Additionally, many factors—physical and psychosocial—can lead to musculoskeletal injuries.
Awkward or prolonged postures generally are considered a major risk factor for work-related musculoskeletal injuries. Although standing upright is considered a safe and neutral posture, completing work on a residential roof requires individuals to assume body positions that are near the extremes of a person’s range of motion. In addition, awkward postures maintained for lengthy amounts of time can increase musculoskeletal injury risk.
Repetitiveness and pace of work also are risk factors and refer to how often a movement or task is repeated and the speeds of the joints during the movements and tasks. Installing residential roof systems is repetitive and happens at a rapid pace. The body is not given time to rest and recover and, over time, will wear down and a musculoskeletal injury could be sustained by a worker.
In addition, many work tasks for residential roofing require high, but not maximal, force loads on the human body. This increases muscle effort, increasing associated fatigue, and when not provided with proper recovery time, can lead to an injury.
Vibration is a musculoskeletal injury risk that is not necessarily predominant for residential roofing workers, but the use of pneumatic tools could create some exposure. During residential roofing work, vibration affects workers’ tendons, muscles, joints and nerves and presents a more localized exposure to the hands. Common symptoms are loss of touch and grip, numbness of the fingers and pain. Furthermore, a worker may use more force and awkward body positions because vibration hand tools are more difficult to control.
Unfortunately, hot and cold weather can increase musculoskeletal injury risks among residential roofing workers. Hot temperatures cause more rapid physical fatigue, which can make workers more vulnerable to injury. In cold temperatures, extremities can become numb, and with numb hands, workers can misjudge the amount of force needed to complete a task. Additionally, cold weather decreases flexibility and increases risk of a musculoskeletal injury.
The musculoskeletal injury risks I mentioned are those that are more biomechanical and physical in nature. There are several psychosocial risk factors that also can contribute to the development of musculoskeletal injuries. Many of these could potentially be associated with residential roofing work.
Psychosocial risks
One psychosocial risk entails a lack of influence or control over one’s job, which occurs when workers feel they do not have any ability to work with supervisors to alter a task.
Increased pressure to be more productive is another common risk in the construction industry. The faster projects are completed, the sooner a worker can be compensated and move on to the next project. The increased speed can lead to mistakes in body posture and increased fatigue.
In addition, when management and workers do not talk to one another, it can lead to a feeling of lack of control of one’s job.
Although psychosocial risk factors might not seem as ominous compared with the risk factors that are biomechanical and physical, all these are important to note. Because of the accumulative nature of musculoskeletal injures, any of these factors—in addition to physical risks—can add up over time.
Each individual worker will respond differently to different stimuli, and it is difficult to create a standard solution for musculoskeletal injury risk. Workers must take the time to learn about the risk factors and be diligent to implement as many procedures as they can to ensure their safety.
Protective intervention
Although protective wearable interventions (such as knee pads, knee savers and extender arms for tools) exist to reduce musculoskeletal injury risk for construction workers, few, if any, exist specifically for roofing workers. One reason for this is the lack of standardization in the residential roofing environment. Other reasons include:
Research
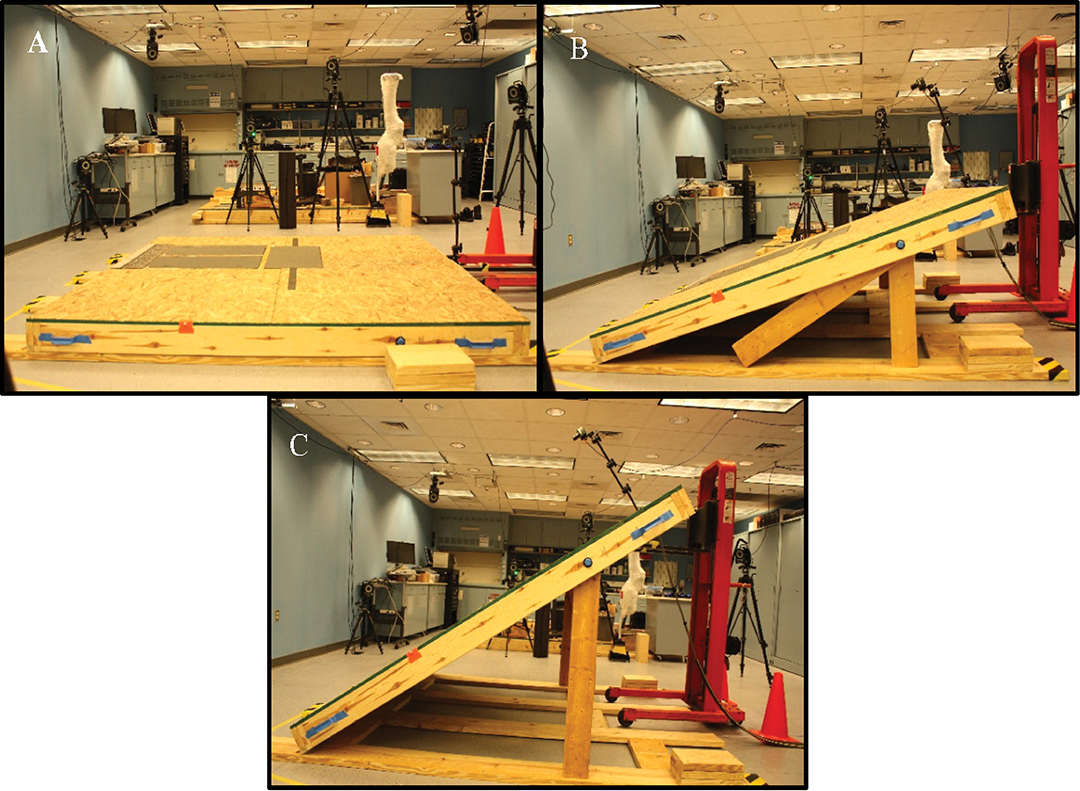
Figure 1: NIOSH’s instrumented roofing simulator segment. The roofing surface can be adjusted from 0 degrees (A) to 15 degrees (B) and 30 degrees (C).
The Physical Effects Research Branch in NIOSH’s Health Effects Laboratory Division initiated a residential roofing research program in 2016 that focuses on reducing musculoskeletal injury risks.
The research uses an instrumented roofing simulator that can be set to multiple pitches to emulate different roofs (see Figure 1). The simulator is a wooden 2 x 6 frame with an oriented strand board walking surface. There are two 2.5- by 2.5-m sections that are placed next to one another to allow more space for gait activities. When the two segments are joined, the roof simulator dimensions are 5 by 2.5 m. One of the sections is instrumented with three force platforms. The force platforms can record ground reaction forces during all the proposed tasks. Both sections of the roof simulator can be locked into three angles: 0, 15 and 30 degrees.
Although this program still is in its infancy, several other studies of musculoskeletal injury risk for residential roofing workers have been completed.
Wearable devices
NIOSH has studied the effectiveness of different wearable devices while kneeling on a slope. Because of the unique work environment, residential roofing workers spend more than 75% of their working time in crawling, squatting, stooping and kneeling postures. The cumulative effects of these awkward postures, combined with repetitive motions, may lead to lower back pain and can increase the musculoskeletal loading in the lower extremities, leading to osteoarthritis.
As a result, roofing workers have the second highest incidence rate of work-related musculoskeletal injuries among all construction sectors and most injuries are observed in the lower back and lower extremities based on BLS data. It was found the introduction of sloped surfaces induces postural changes—particularly in the side view—of kneeling workers that prompts an awkward posture, which may lead to increased injury risk.
Knee savers reduce the extreme posture during workers’ resting positions. But the study concluded knee savers—despite not being designed for use on a sloped surface—also were able to stimulate a more neutral posture in workers’ knees and hips. Although it is promising wearable devices are effective, current models NIOSH tested might not alter posture enough to have a clinical effect on musculoskeletal injury risks for roofing workers. Therefore, this project was a first step in using roofing-specific wearables to reduce these risks, and a future project should focus on optimizing knee savers for roofing-specific activities.
Knee disorders
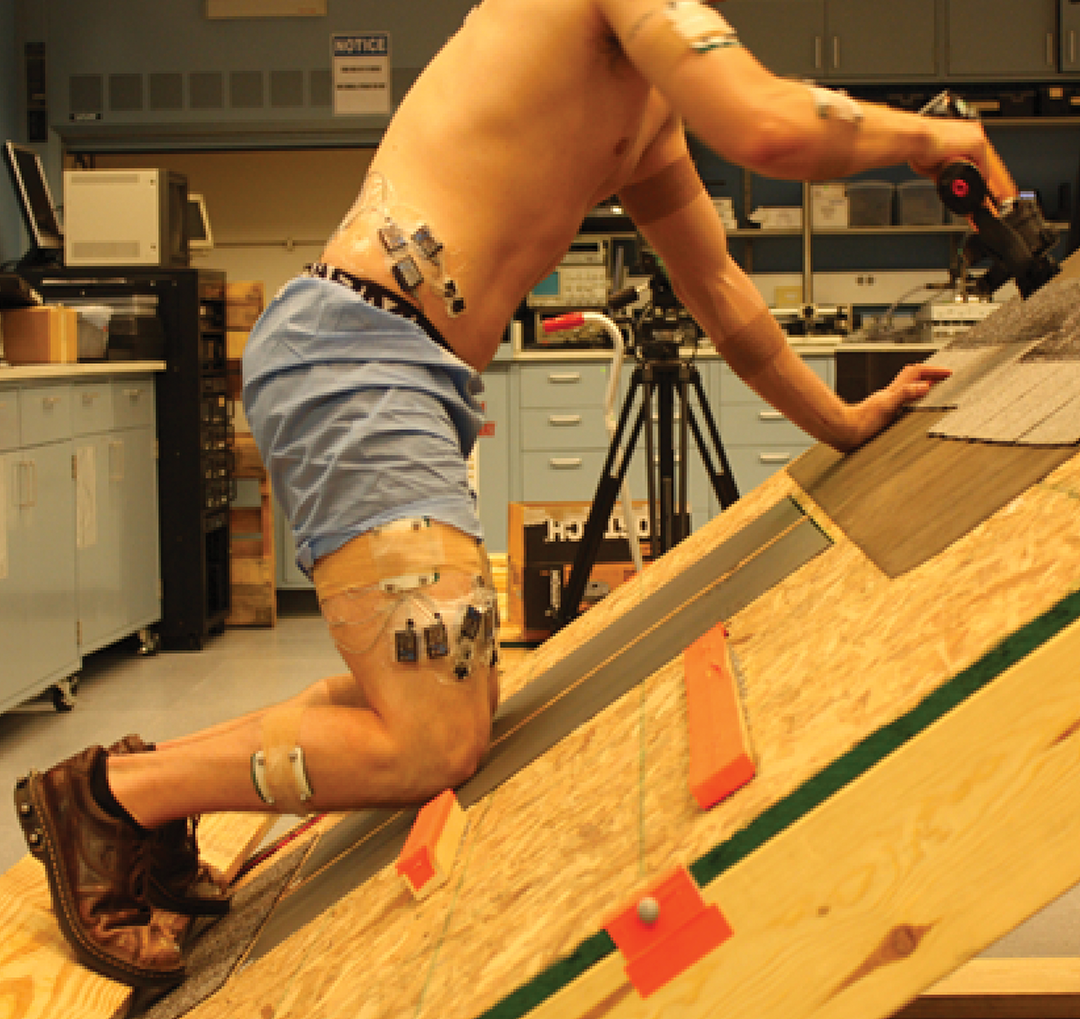
Figure 2: Subject kneeling on an instrumented roof segment
Roofing workers often suffer from musculoskeletal injuries in their knees, and several ergonomic studies have identified kneeling as a potential risk factor for knee injuries and disorders. To assess work-related injury risks caused by kneeling during shingle installation, NIOSH used its pitch-configurable roofing simulator (see Figure 2). This study found roof pitch and working posture significantly affect developing musculoskeletal injuries among roofing workers. Roofing workers become more exposed to knee injury risks working in a dynamic kneeling posture during shingle installation than in a static kneeling posture. The study also found that though certain musculoskeletal injury risk factors are reduced on a high-pitched roof, other musculoskeletal injury risk factors on high-pitched roofs increase during shingle installation. Therefore, proper attention is required when working on high-pitched roofs during shingle installation.
Body motion
In another study, subjects traversed across a 26-degree roof segment during which lower extremity 3D body motions were calculated. One foot was higher on the slope, and the other was lower for the duration of cross-slope walking. Overall, cross-slope walking on a 26-degree roof significantly altered 77% of the measured peak lower extremity variables compared with level self-selected pace walking.
The data suggests roof pitch incites significant differences in cross-slope walking and these alterations could temporarily alter body position sense, which may lead to increased falls and musculoskeletal injury. This study only quantified the changes from a level condition to a sloped condition. The changes in lower extremity variables cannot be classified as good or bad until further investigation is conducted.
Stilts walking
Construction workers often use stilts to reach a higher level above ground to perform many tasks. Some epidemiological studies indicate the use of stilts may place workers at increased risk for knee injuries and/or increase the likelihood of trips and falls.
In the NIOSH study, we developed an inverse dynamic model of stilts walking to investigate the effects of this activity on the joint moments and musculoskeletal loadings in the lower limbs. The stilts-walk model was developed using the commercial musculoskeletal simulation software AnyBody.
Simulations were performed using data collected from tests of four subjects. All subjects walked without or with stilts through a 12-m straight path. The simulations showed the use of stilts may potentially increase the peak joint rotational force in knee extension by about 20% and induce 15% reduction and slight reduction in the peak joint moments in ankle flexion and hip extension, respectively.
The model predictions on the muscle forces indicated the use of stilts may potentially increase loadings in five of eight major muscle groups in the lower extremities. The most remarkable was the force in one of the quadriceps muscles, which was found to potentially increase by up to 1.79 times for stilts walking compared with that for normal walking. This model would be useful for engineers in their efforts to improve stilt design to reduce musculoskeletal loadings and fall risk. Although stilts are not used for residential roofing surfaces, many of the musculoskeletal methods developed in this study are readily transferable to the study of roofing workers’ musculoskeletal injuries.
Low-back disorders
Roofing workers have long suffered from low-back disorders. These workers spend more working time kneeling, stooping, crawling and squatting on slanted rooftops compared with working on flat ground; consequently, they are constantly bending or twisting their bodies. NIOSH has investigated the effect of uneven ground surface on lower back injuries during the performance of manual material handling tasks. The results suggest that when a worker performs manual material handling tasks, a slanted surface changes trunk biomechanics, potentially resulting in elevated spinal loading and lower back pain.
NIOSH’s simulated roof shingle installation was analyzed in four sequential phases:
Many differences were observed between slope and phase, but one interesting result is that as the pitch of a roof increased, the maximum flexion angle of the worker’s trunk decreased. The results suggest trunk posture is influenced by differences in roof pitch and shingle installation tasks and devices such as knee pads and knee savers may reduce joint angles in the trunk; however, there are no such devices currently designed exclusively for roofing work.
Deep squatting
Expanding and using the musculoskeletal modeling methods from the stilts project, NIOSH also investigated the knee muscle response during deep squatting (120 or more knee bends) with and without knee pads. It was observed that the use of knee pads helps reduce normal contact forces on the inside and outside of the knee joint 42% and 57%, respectively. Although these results are promising for reducing musculoskeletal injury risk for residential roofing workers, more work needs to be done to understand how to reduce this risk.
Bottom line
Residential roofing work creates an environment that exposes workers to an increased risk for musculoskeletal injuries. Research at NIOSH is intended to develop and help implement guides for employers to establish effective workplace programs that sustain and improve worker health. Employers are accountable for ensuring safe working conditions and guaranteeing workers are using safe work practices. We encourage employers to develop training programs to bring awareness to employees to help minimize musculoskeletal injury risks on residential roofs.
Scott P. Breloff, Ph.D., is a NIOSH biomedical engineer.
COMMENTS
Be the first to comment. Please log in to leave a comment.